GCS/SRS Techniques Overview
How Surgeons Around the Globe Perform GCS/SRS
According to Dr. Kaushik, in our age and time, a surgeon’s goal of successful FtM GCS/ SRS should meet the following criteria:
- create a naturally looking vulva with all regualar aspects of a female vulva
- create a fully sensate clitoris with a natural appearance and orgasmic capability
- create a vagina which remains patent (stays this way) till the maximum possible depth
- the vagina should be fully vascular, fully sensate, and fully functional
- the vagina should have a lubrication lining which generates proper lubrication on sexual arousal
- the vagina should enable natural sexual intercourse and hopefully vaginal orgasms
The following list briefly explains and compares surgical vaginoplasty methods as they became popular in chronological order
1.) Penile Inversion (PI) GCS/ SRS
Dr. Kaushik’s nowadays considers PI GCS/SRS to be a purely Cosmetic GCS/SRS surgery because the emphasis is to create proper external genitalia – a vulva – in analogy to the common fetal tissue base and its differentiation into female or male outer genitalia. Working alongside this guideline, very cis-like female outer genitalia structures can be created, as long as the focus on using penile skin for a vaginal lining is obliterated and the focus is kept on using them for vulva creation.
Very little skin is used to create a vaginal opening and a non-functional “vagina” of 1-2 inches only – which Dr. Kaushik defines as Cosmetic GCS/SRS.
This vaginal opening can be connected to a Sigma-Lead graft at a later time. All of Dr. Kaushik’s Cosmetic GCS/SRS patients, who want to enjoy natural sexual intercourse after their Cosmetic GCS/SRS can opt for the Sigma-Lead CompletionGCS/SRS in order to have a fully functional, naturally deep, self-lubricating, and sensate vagina.
Patients who already underwent PI SRS/GCS but lack vaginal depth, proper vagina function, or whose neovagina has closed itself completely, can have Sigma-Lead Revision GCS/SRS with excellent results in the form of a naturally deep, lubricating, and sensate vagina.
2.) Advanced Penile Inversion Technique/ Penile Inversion With Scrotal Graft Technique
In quite a number of patients the penile skin available will be insufficient for a full-length penile skin neovagina.
To gain extra depth, a full thickness or split thickness skin graft from the scrotum and/or the groin is used. This way, good vaginal depth of 4-5 inches can be achieved in almost every case. Drawbacks are the chances of loss and/ or shrinkage of the skin graft leading to depth and diameter restrictions. These healing issues can only be counteracted by absolutely mandatory, prolonged, painful, and cumbersome dilation.
Basically, the skin graft/ skin flap itself is a low-quality choice for vaginal lining for numerous reasons.
The glandular skin components of the sweat and sebaceous glands lead to secretions that get collected over regular intervals and often lead to unregular, smelly, and often pus-like discharge. Also, quite a number of patients hair growth problems within the vagina.
Intense lubrication using intimate gel is required for proper intercourse. The timeconsuming dilation regimen often cannot be upheld while patients try to follow regular work and try to maintain a normal social life.
We here at Olmec can confirm that Sigma Lead revision rates for former advanced PI/ scrotal graft PI have gone up drastically. The PI-Scrotal Graft GCS/SRS technique should no longer be the first choice for MtF transgender individuals.

3.) Full-Length Full-Thickness Scrotal Skin Graft SRS
The basic idea of the full (scrotal-) graft vaginoplasty was to overcome the limitations of the penile inversion SRS/GCS which stems from inverting the valued penile skin and using all or a big part of it to line the vagina with it. Also, it is geared to provide for a tension free vulva/ vagina setup.
To improve cosmetic appearance, it was necessary to use more penile skin and preputial skin to create the various vulva parts. The full scrotal graft GCS/SRS approach allowed the surgeon to create cis-like labia minora, clitoral hooding and clitoris, and labia minora extending all the way down to the vaginal opening. No penile skin was used to line the vagina. A complete full-length fullthickness scrotal graft is used to line the vagina. It gets freed of most hair follicles hoping to create a hair free vagina and it gets sutured to the perineum and the outer penile skin.
This technique overcomes the cosmetic limitations for vulva creation of the surgical penile inversion variants, but it further increases and complicates the limitations a skin graft has, making dilation an even more substantial, more painful, and more time-consuming process compared to basic penile inversion technique.
That is why, in Dr. Kaushik’s opinion, MtF transgender individuals should avoid this GCS/SRS surgery technique.

4.) Peritoneum GCS/SRS Surgery
Surgeons began to use this approach for CIS-female MRKH patients since 1974 and it was usually performed as a pull-through procedure.
Only in recent years have surgeons begun to adapt this technique for transgender women. The peritoneum is a suitable alternative to any skin graft GCS/SRS due to its abundant availability, its closeness to the vaginal cavity, its mucosa-type (squamous epithelium cell) surface, and its ability for lubrication. Whenever Sigma-Lead GCS/SRS is not possible -for whatever reason – the peritoneum GCS/SRS is the second best option for all transgender women who want GCS/SRS.
The peritoneum itself is not as trauma-resistant as a colon graft and doesn’t have that room-space and wall thickness ratio of a Sigma-Lead graft.
The big plus compared to the Sigma-Lead GCS/SRS is, that no anastomosis with its adherent risks needs to be performed.
5.) Sigmoid Colon GCS/SRS
Sigmoid colon vaginoplasty was designed to overcome the limits of penile inversion, advanced PI skin-graft, full-length scrotal graft, and peritoneal GCS/SRS techniques.
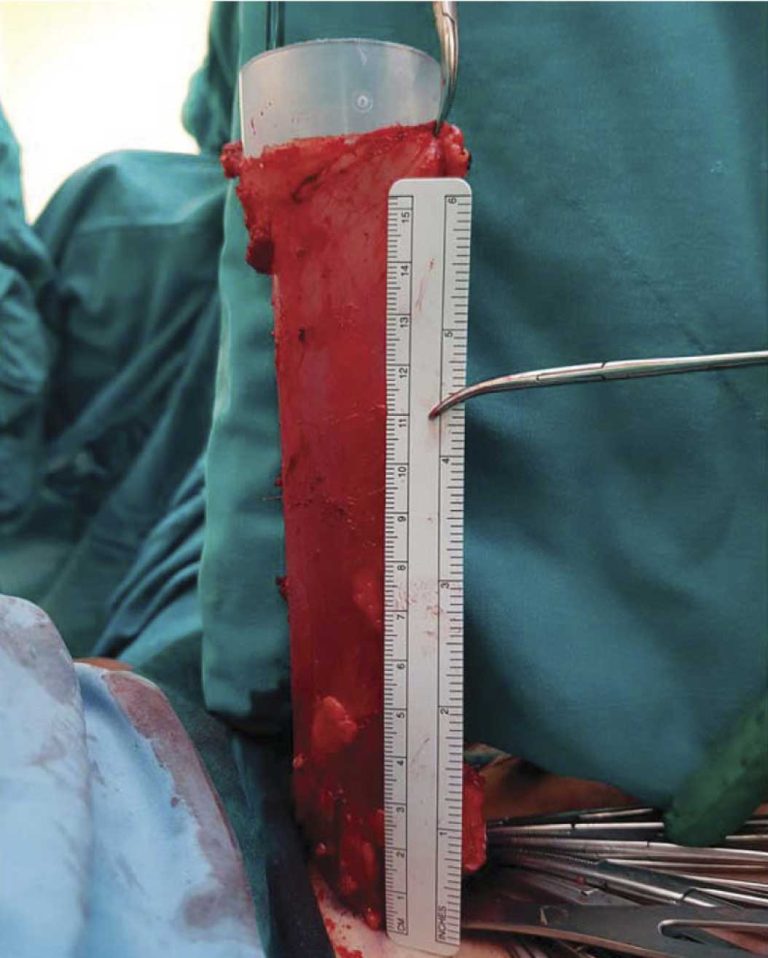
A proper-length segment of sigmoid colon with its attached blood supply is used as the neovagina. The sigmoid colon graft is sutured close at one end. The open end of the sigmoid colon graft is sutured to the vaginal opening skin in around 1-2 inches (2 – 4 cm) of depth. The result is a fully deep, naturally lubricating, and sensate vagina.
The aspect of suturing inside the vagina avoids the visibility of the red mucosa of the colon graft at the vaginal opening, which was an issue in the first sigmoid colon GCS/SRS surgeries in the 1970’s and 1980’s. Also excessive prolonged vaginal discharge because of the secretions of a too-long segment of the colon or an improper sigmoid colon graft choice is nowadays a thing of the past. In earlier times, the need of prolonged dilation was sometimes necessary to keep the vaginal opening patent. The reason for that was that the junction of normal perineal skin and the colon graft sutured to it tended to contract. Nowadays this is also a thing of the past for any experienced and well-trained sigmoid colon GCS/SRS surgeon.
6.) OLMEC SIGMA-LEAD GCS/SRS
This advanced type of sigmoid colon SRS/GCS is exclusively practiced at OLMEC and has become the technique of choice and thus the gold-standard for all of Olmec’s MtF transgender individuals.
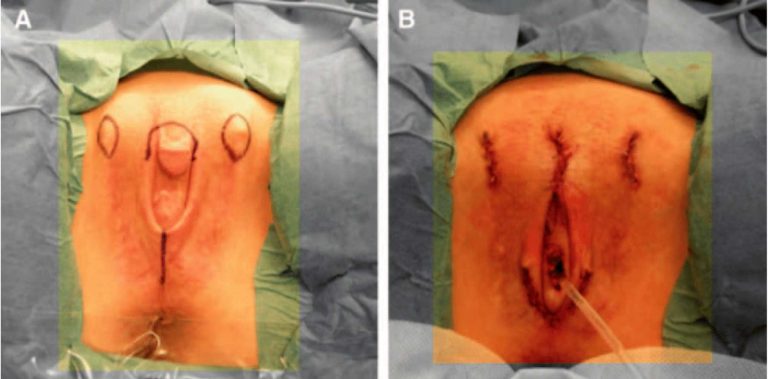
The valued penile skin can be used accordingly to create wonderful, cis-like outer female genitalia without compromise since there is hardly any penile skin needed for the vaginoplasty.
In this technique, the first portion of the introitus – the vaginal opening – (about 1 to 2 inches/ 2-4 cm) gets lined with penile skin and this skin is then sutured to the sigmoid colon graft. All tissues that are being used for the creation of the vagina – the small part of the pedicled penile skin and the pedicled sigmoid colon graft – have their own blood and nerve supply
This ensures complete sensation of the area and guarantees an enormously fast healing procedure. The regular depth of the SigmaLead vagina is 7 to 10 inches (17 – 25 cm) deep and the vagina is fully sensate with a self-lubricating lining upon sexual arousal. This fully functional deep vagina assists in natural orgasms during masturbation as well as during sexual intercourse. The vaginal opening (introitus) looks natural. The colon graft length needed is small. Hence the part utilized is restricted to the distal sigmoid colon, also known as rectosigmoid colon. This bowel part is known to produce minimum secretions, hence the problem of excessive secretions is a thing of the past.
Another most valuable part is minimum post-operative care and shorter dilation time periods and intervals because the zigzag suture pattern at the concealed junction of soft penile skin and sigma-lead graft has minimum chances of contraction.
Having performed all techniques over the last 14 years, Dr. Kaushik pretty soon has come to the conclusion that the fastest and best result for a TS*woman wanting GCS/SRS are achieved with his OLMEC SIGMA-LEAD SRS/GCS technique.
This procedure has consistently delivered superior overall results, both aesthetically and functionally.
Every Olmec Sigma-Lead patient will confirm that she has the experience of her genitals feeling like a natural vulva and vagina to her within a short time after surgery.