A Brief History of GCS/ SRS
For thousands of years the hjras in India have been performing what could be labelled as the first – yet quite incomplete – genital reassignment surgery in history. They call it nirvan or nirwaan and it consist of the removal of the penis and the testes. Still practiced today, though it is officially banned, it shows that the 3rd gender has been part of Indian life and society ever since Hinduism existed, since these rites stem from the hinduistic vedas. Only when the English invaded India this part of Indian society was banned and forced to go underground because it was declared inappropriate, unfit and unnatural.
In 1930 Germany’s unknown Dora R was the first person in history to undergo a highly experimental vaginoplasty by Dr. E. Gehrbrandt.

Also in 1930 and 1931 German surgeons Dr. Ludwig Levy- Lentz and Kurt Warnekros performed various procedures on the first famous recipient of GCS/SRS in history, Danish intersex individual Lili Elbe, born Einar Wegener. Due to Nazi reign and action, most of the documents of the procedures Dr. Warnekros performed on Lili Elbe got destroyed. Ultimately Lili Elbe died of cardiac arrest in September 1931 being a complication of the uterus transplant she received. Ciclosporin, the drug that could have saved her life, first came into use to prevent rejection of transplanted organs in 1980 – 50 years later.
It was in 1956 when modern GCS/SRS saw the light of day when French gynecologist Dr. Georges Burou had the idea and successfully performed the first pedicled penile skin inversion vaginoplasty in his Clinique du Parc in Casablanca, Morocco.
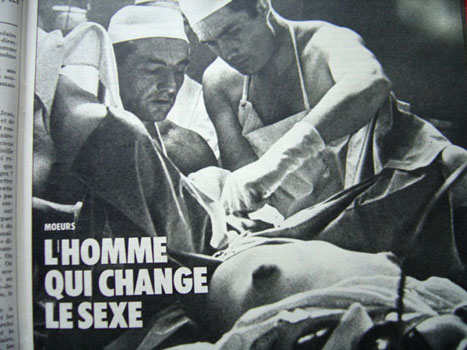
Dr. Burou’s vaginoplasty uses life penile skin grafts to construct a neovagina. He gained growing publicity and popularity after an article of the French magazine France Dimanche about a French carpenter who underwent successful GCS/SRS with Dr. Burou was published. It drew hundreds of patients from all over the world to his Clinique du Parc and within the next 30 years more than 3000 patients received GCS/SRS surgery by Dr. Burou in Casablanca.
His famous quote, said at the first official presentation of his GCS/SRS technique at a symposium at Stanford University in Stanford, California, USA in 1973 shows, how much in perspective and how true Dr. Burou saw his role as being a plastic surgeon for MtF transgender individuals:
I do not transform men into women.
I transform male genitals into genitals that have a feminine aspect.
All the rest is in the patient’s head.
In 2001 full-length full-thickness scrotal graft vaginoplasty got first performed by Dr. Suporn in Thailand and set a new standard in cosmetic appearance. At the same time, this procedure was also setting a new threshold challenge for the duration of post-op aftercare and for painful post-op care dilation routines. The core idea was to use all of the valued penile skin to create the vulva – the external female genitals. The vagina is made up of a thin full-length full-thickness scrotal skin graft. This way the depth of the vagina was independent of penile length while still inheriting all the negatives of a regular skin graft, which is the reason for the usually long and painful post-operative healing phase.
Another surgical option re-entered the stage in the 1970’s: colon vaginoplasty.
Bowel vaginoplasty was first described by Sneguireff in 1892 to treat vaginal agenesis (absence of a vagina in female patients). In 1904 Baldwin was the first to describe a small bowel surgery to create a vagina and also suggested the sigmoid colon might be suitable for that procedure. Yet these procedures got abandoned at that time because of the high complication rate.
In 1974 Markland and Hastings used cecum and sigmoid transplants for their colon vaginoplasties. The need to cure agenesis in women affected the situation and also the idea to use that concept for MtF transsexual individuals made surgeons have a look at this surgical approach again.
New medical techniques, concepts, medication, and suturing possibilities made this approach the most promising alternative in the surgical field. Even a recent study by the University of Gent in 2015 promoted by Prof. Dr. Stan Monstrey concludes that intestinal vaginoplasty is a safe technique and Kim et al. recently concluded that rectosigmoid vaginoplasty is the best choice for male to female transsexuals who have previously undergone total penectomy (removal of the penis) and orchiectomy (removal of the testes), or for those with previously failed skin vaginoplasty and for patients with Mayer- Rokitansky-Kuster-Hauser syndrome.
New medical techniques, concepts, medication, and suturing possibilities made this approach the most promising alternative in the surgical field. Even a recent study by the University of Gent in 2015 promoted by Prof. Dr. Stan Monstrey concludes that intestinal vaginoplasty is a safe technique and Kim et al. recently concluded that rectosigmoid vaginoplasty is the best choice for male to female transsexuals who have previously undergone total penectomy (removal of the penis) and orchiectomy (removal of the testes), or for those with previously failed skin vaginoplasty and for patients with Mayer- Rokitansky-Kuster-Hauser syndrome.
“We suggest sigmoid colon vaginoplasty as a better treatment modality because of its large lumen, thick wall resistant to trauma, adequate secretion allowing lubrication, not necessitating prolonged dilatation, and short recovery time.”
An example of how wrongly the sigmoid colon procedure was judged about 11 years ago can be found on this discontinued website called GID info (Gender Identity Disorder), which shut down operations in May 2005:
Sigmoid Colon Vaginoplasty – This operation was adapted from a procedure performed on intersexed and underdeveloped girls who were born without vaginas. There are much greater risks to undergoing this surgery because the abdominal cavity is entered and the patient must concurrently heal from TWO major operations at the same time.
Unfortunately, such information is still around without reflecting all the advancements that have come about in eleven years of medical and surgical progress. Such information oftentimes gets repeated in forums. Forums unfortunately also don’t reflect all the progress that is being made in the medical and surgical field, Let’s say someone says they got sigmoid colon SRS/GCS 15 years ago, that will not reflect the state of the art performance of such treatment that can be achieved today.
And on a side note, full-length graft vaginoplasty had just emerged from its cocoon at that time.
OLMEC SIGMA-LEAD SRS/GCS
Dr. Kaushik created his unique and innovative techniques in the form of Peri-sanstuary Peritoneal Vaginoplasty and Sigma Lead (sigmoid colon) Gender Affirmation techniques, which combine various elements from all major surgical SRS/GCS techniques where he sees fit.
The first and uppermost principle he adheres to is: pedicled tissue, wherever possible! Pedicled tissue means the tissue has its own blood and nerve supply. This is THE major factor for graft and tissue survival and for a fast and safe recovery.
Whenever some tissue gets transplanted Dr. Kaushik puts uppermost care on using the tissue’s blood supply to ensure maximum graft survival.












